Bioluminescence imaging (BLI) is a non-invasive optical imaging modality designed to visualize and quantify bioluminescent signal in tissues.1 BLI is based on the detection of visible light produced during enzyme-mediated oxidation of a substrate when the enzyme is expressed in vivo as a molecular reporter.
BLI offers a robust, sensitive and high throughput alternative relative to more traditional imaging and biodistribution studies using terminal endpoints, invasive procedures or radiolabeling. We were the first CRO to offer BLI in 2003 and in the 17 years since we have amassed considerable experience and know-how in this optical imaging field. In this Technology Spotlight we will present the principles of bioluminescence imaging and highlight advantages this preclinical service offers in cancer detection, monitoring disease progression and in vivo anti-tumor efficacy assessment.
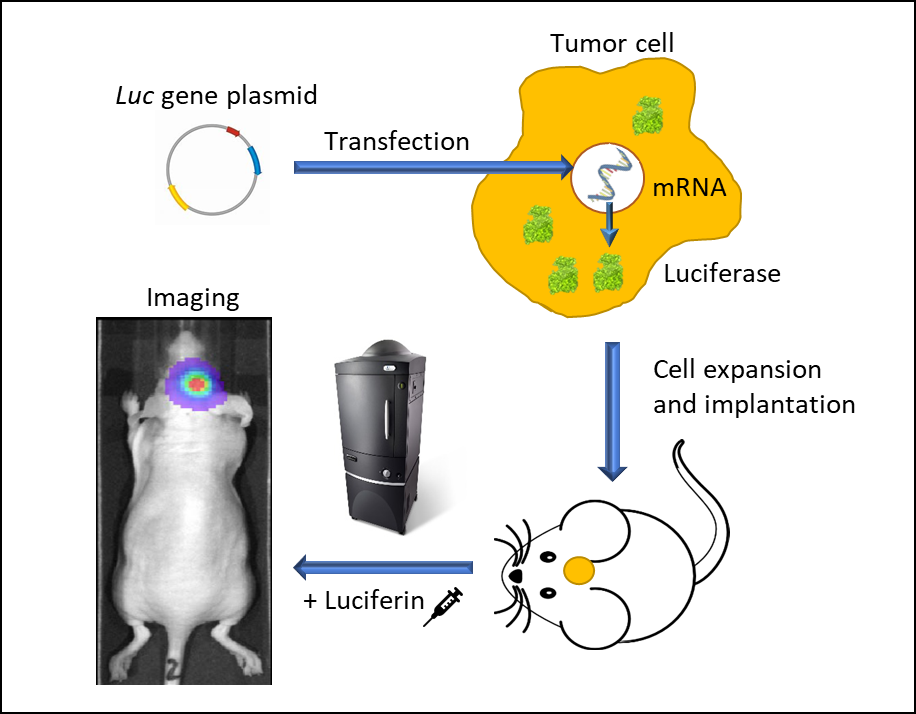
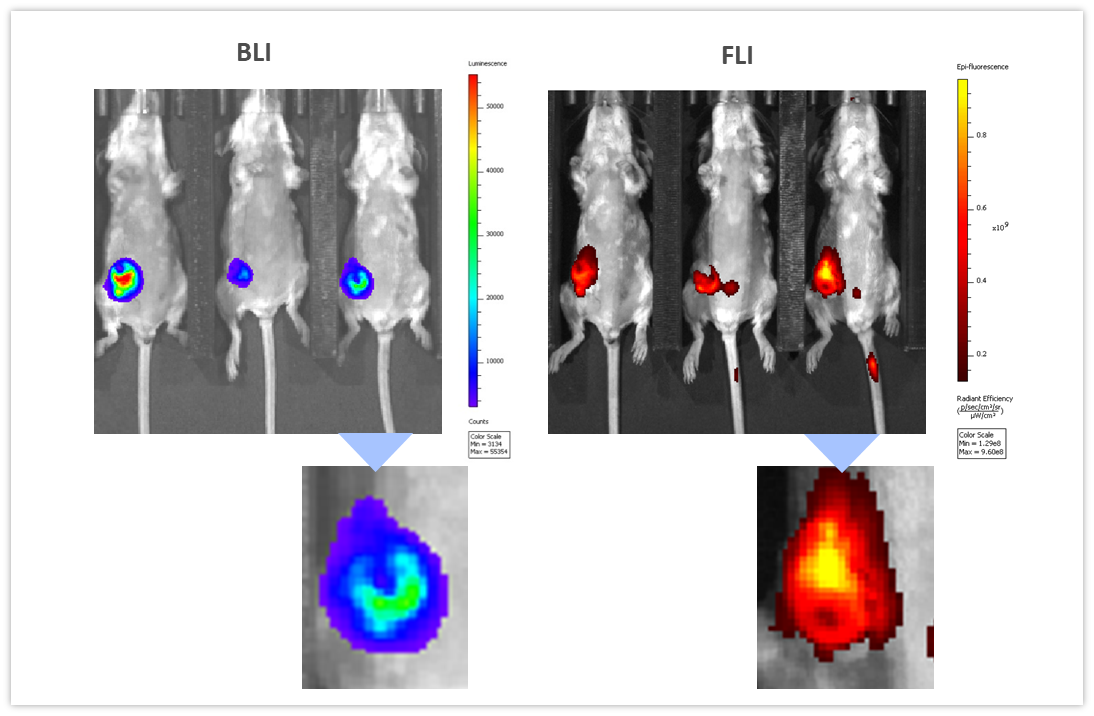
BLI requires cells to express luciferase, a word suitably derived from the Latin lucifer—lightbringer, produced for example by fireflies or sea pansies. The firefly luc gene was first cloned in 19852 and since, green is the most used fluorescence color imaging. Firefly luciferase requires the injection of its substrate, D-luciferin which generates a bioluminescent signal peaking at 562 nm, captured by a high quantum efficiency charged coupled device camera (CCD) placed in a light-tight cabinet. The sequence of events leading from engineering tumor cells to express luciferase to imaging animals in vivo is illustrated in Figure 1. We use IVIS® In Vivo Imaging Systems (PerkinElmer, Waltham, MA) which allow high sensitivity and high resolution in vivo BLI and fluorescence imaging (FLI) across a wide range of wavelengths. Animals are imaged up to five at a time under 2% isoflurane gas anesthesia. Each mouse is injected with D-Luciferin and imaged 10-15 minutes after the injection. BLI signal is quantified in regions of interest (ROIs) drawn around tumors, specific areas (for example cranial, thoracic or abdominal), whole body or tissues ex vivo and the signal is expressed as photons per second, representing the flux radiating omni-directionally from the user-defined region. Images are analyzed using Living Image 4.3.1 (PerkinElmer, Waltham, MA) software.